
Researchers in a 2026 meta-analysis combined the results of 11 randomized trials and found that natural FETs were associated with slightly higher live birth rates and lower miscarriage rates than medicated FETs in women who ovulate regularly.
Frozen embryo transfer (FET) can be performed after preparing the endometrium in different ways. The two most common approaches are a natural cycle, where ovulation occurs naturally (with or without an hCG trigger), and a medicated cycle, where estrogen and progesterone are used to prepare the lining.
Medicated cycles are more flexible for scheduling and are often used for women who don’t ovulate regularly. However, the corpus luteum is preserved in natural FETs, which produces progesterone and other factors that support implantation, placental development, and early pregnancy.
Previous studies have reported conflicting results, making it unclear whether one approach leads to better pregnancy outcomes.
A new meta-analysis by Lin et al. (2026) combined 11 randomized controlled trials (RCTs) to see whether one method leads to better pregnancy outcomes than the other. Because it included only RCTs, it provides the highest-quality evidence currently available for this question.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study design: Systematic review and meta-analysis of 11 randomized controlled trials published between 2015 and 2026
- Risk of bias: The authors judged one study as having low risk of bias, five with some concerns, and five with high risk of bias.
- Participants: 9955 women undergoing FET (5227 had a natural FET, 4728 had a medicated FET). The average maternal age ranged from 28.5–38.7 years.
- Natural FETs included both true natural cycles (spontaneous LH surge) and modified natural cycles (hCG trigger). Medicated FETs used estrogen and progesterone, with some studies also using GnRH agonists.
- Studies included both blastocyst and cleavage-stage transfers, single and multiple embryo transfers, and both PGT-A and non-PGT-A cycles.
- Only intention-to-treat analyses were included.
- Primary outcome: Live birth rate
Natural cycles showed better overall pregnancy outcomes
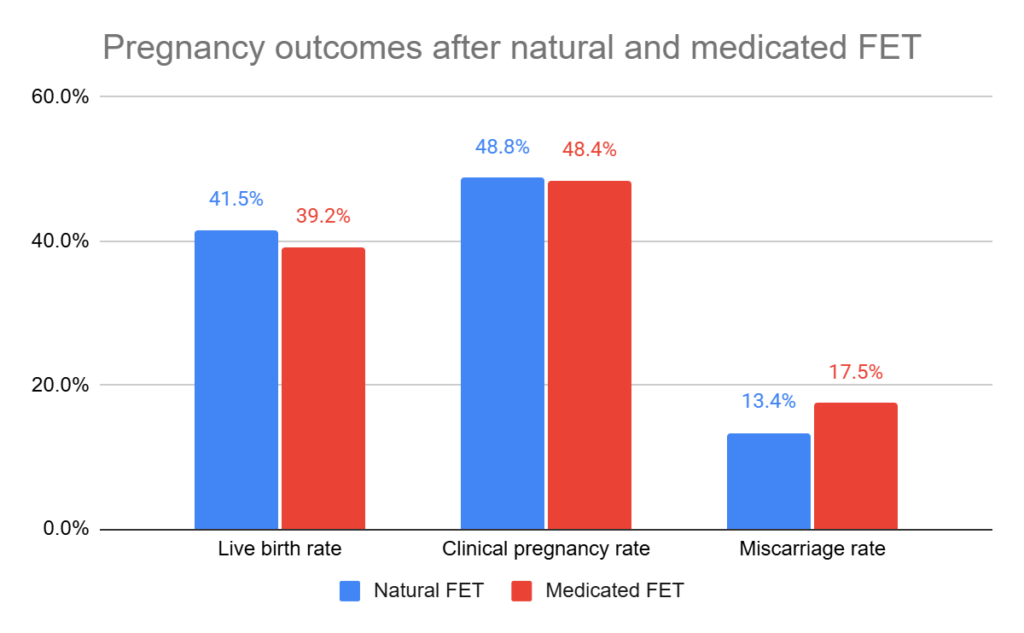
Across all 11 randomized trials, women undergoing a natural FET had slightly better pregnancy outcomes than those undergoing a medicated FET.
- Live birth: 41.5% vs 39.2%
- Risk ratio [95% CI]: 1.11 [1.03–1.19] (p= 0.007, 9955 participants, I2= 27%). This means that women who had a natural FET had an 11% higher relative chance of live birth than those who had a medicated FET. Note that this is a relative, not absolute, increase. For example, an 11% relative increase from a 50% live birth rate corresponds to an absolute increase of 5.5 percentage points (from 50% to 55.5%).
- Clinical pregnancy: 48.8% vs 48.4%
- There was no statistically significant difference between natural and medicated FETs (RR [95% CI]: 1.02 [0.98–1.06], p= 0.40, 9955 participants, I2= 0%).
- Miscarriage: 13.4% vs 17.5%
The authors estimated that using a natural FET instead of a medicated FET would result in about 33 additional live births per 1000 women treated, with one additional live birth for every 31 women treated.
Subgroup analyses suggested that the improvement in live birth rates was mainly driven by modified natural FETs:
- Modified natural FETs were associated with a higher live birth rate than medicated FETs (RR [95% CI]: 1.11 [1.01–1.23], p= 0.04, 8 studies, 3801 participants, I2= 0%).
- There was no statistical difference between true natural and medicated FETs (RR [95% CI]: 1.09 [0.96–1.24], p= 0.19, 4 studies, 1866 participants, I2= 0%).
There was no difference in the rate of cycle cancellation for natural vs medicated FETs (15.6% vs 11.1%, risk ratio [95% CI]: 1.13 [0.73–1.75], p= 0.58, 9 studies, 9287 participants, I2= 87%).
The results were generally consistent
The researchers repeated their analyses in several different ways (called sensitivity analyses) to see whether the results changed. For example, they looked at how live birth rates changed when they excluded studies that did PGT-A, or used cleavage stage embryos, etc. Overall, the findings remained similar, increasing confidence that the results were reliable and not driven by one particular group of patients or treatment protocol.
However, one important limitation is that the researchers didn’t repeat the analysis after excluding the studies judged to be at high risk of bias. This type of sensitivity analysis helps determine whether the overall findings remain the same when only the most reliable studies are included. Without it, it’s hard to know how much the higher-risk studies influenced the results.
Conclusions
After combining the results of 11 RCTs, this meta-analysis suggests that natural FETs were associated with slightly higher live birth rates and lower miscarriage rates than medicated FETs, increasing live birth rates from 39.2% to 41.5%, corresponding to approximately 33 additional live births per 1000 women treated.
These results were consistent even after repeating their analysis in several different ways.
The benefit was most obvious with modified natural FETs. True natural FETs didn’t show a statistically significant improvement, but the estimated benefit was very similar. More research directly comparing modified and true natural FETs is needed to determine whether one approach is actually better than the other.
There wasn’t any significant difference in cycle cancellation rates, although there was a high amount of variability between the studies (I2= 87%), so this result is less reliable.
Unfortunately, this study didn’t look at adverse pregnancy outcomes (like preeclampsia), which some studies show are higher with medicated FETs.
One possible explanation is the presence of the corpus luteum in natural cycles. In addition to progesterone, the corpus luteum produces hormones and signaling molecules such as relaxin and VEGF, which may help support implantation, placental development, and early pregnancy. Medicated cycles lack a corpus luteum, which may partly explain both the lower live birth rate seen here and previous research linking medicated cycles with higher rates of hypertensive disorders during pregnancy.
The authors conclude that natural FETs may be the preferred option for most women who ovulate regularly. However, they emphasize that treatment should be individualized. Medicated FETs remain an important option for women who don’t ovulate regularly, are using donor eggs, or prefer a more predictable treatment schedule with greater scheduling flexibility.
Limitations include the high risk of bias in nearly half of the included trials, differences in treatment protocols between studies, the relatively young age and good prognosis of most participants (which may limit how well the findings apply to all IVF patients), and high variation in cancellation rates between clinics. Despite these limitations, this meta-analysis represents the highest-quality evidence currently available because it included only RCTs.
Want to read more about natural FETs?
A 2026 meta-analysis explored ways to optimize natural FETs, examining ovulation timing, progesterone use, luteinized unruptured follicles, and cycle variability across natural, modified natural, and newer natural proliferative phase approaches. Read more.
Researchers in a 2023 study found decreased adverse pregnancy and neonatal outcomes in those who performed a natural vs medicated FET, including abnormal birth weights, preeclampsia, preterm births, and more. Read more.

Researchers in a 2026 randomized controlled trial found that natural FETs using euploid embryos were associated with lower early pregnancy loss rates and higher live birth rates than medicated transfers, although the study was stopped early. Read more.
Researchers in a 2022 study compared timing of euploid transfers and found that 160 h was optimal for modified natural FETs, while they found no optimal time for natural FETs. Read more.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.